Vitamin E – the good and the bad
December 10. 2024
Vitamin E is a large family of active substances, with alpha-tocopherol being the most well-known and used, but it has good and bad relatives.
Atherosclerosis and cardiovascular disease are some of the most common causes of death worldwide, and also reduce the quality of life for millions of people. The authors of a new article have reviewed the recent scientific evidence on the effects of increased intake of the two main forms of vitamin E, tocotrienols and tocopherols, on patients with atherosclerosis and the cardiovascular diseases that accompany atherosclerosis (Rafique et al., 2024).
The article has focused on the fact that vitamin E is much more than the commonly known alpha-tocopherol, and that some of the other forms of vitamin E in the diet may contribute to better protection of the body’s cardiovascular system.
An attempt to illustrate the structure of vitamin E can be seen below, where the four tocotrienols are on the left with three double bonds in the long carbon chain, and the four tocopherols are on the right.
Tocotrienols Tocopherols
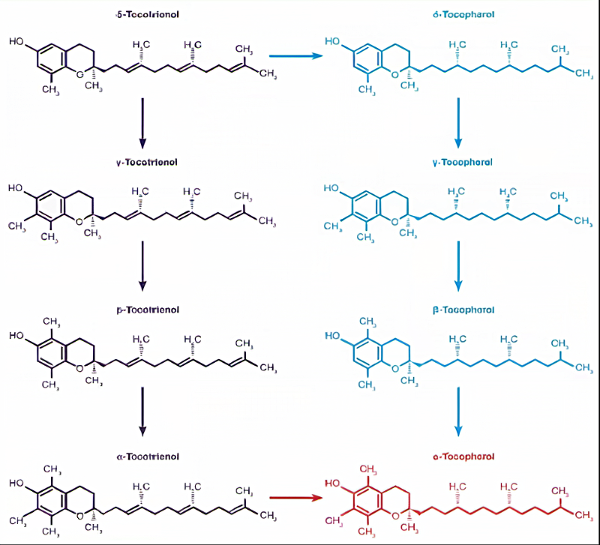
Figure 1: The eight substances that naturally belong to the vitamin E group in plants. The tocotrienols are on the left, and the tocopherols on the right. Alpha-tocopherol is shown in red. The arrows in the figure show how trienols can be converted to alpha-tocopherol in our body. (Figure modified from Querchi et al. (2015)).
The new article is based on a review of 5 studies published in the 8 years from 2015-2022, which examined the effect of tocotrienol or tocopherol supplementation on the development of atherosclerosis or patients with already existing atherosclerosis and other cardiovascular diseases.
A study highlighted in the recently published article showed that tocotrienol at a dose of 250 mg per day for 16 weeks had a clear positive effect on reducing cholesterol and reducing important biomarkers of oxidative stress and inflammation in the body (Querishi et al 2015):
- C-reactive protein (CRP): a 40% decrease
CRP is produced in the liver and is a frequently used marker for inflammation in the body in general and also for atherosclerosis, where a lower level gives patients a lower risk of having a blood clot.
- Malondialdehyde (MDA): a decrease of 34%
Malondialdehyde is produced in the body’s tissues and high levels are a sign of oxidative stress and low antioxidant levels.
- Gamma-glutamyl transferase (GGT): a decrease of 22%
High GGT levels in the blood are a sign of strain on the liver-biliary system and pancreas.
Along with the above positive changes, the total antioxidant status in the blood was increased by 22%, and cytokines that promote inflammation, such as interleukins (IL-1, IL-12), were reduced by 15-17%. Tocotrienol also had a positive effect on several types of micro-RNA, which are important in the regulation of inflammation and fatty acid metabolism.
Overall, the article showed that tocotrienol can help reduce the processes in the body that lead to atherosclerosis – especially in patients with already existing symptoms of cardiovascular problems.
However, the positive studies on tocotrienols mentioned in the new article are all of shorter duration – 3–6 months. In contrast, the studies the article compares with were all conducted with alpha-tocopherol, and of duration as long as 30 years.
These long-term studies of alpha-tocopherol have shown results with considerable variation. A Finnish study (Huang et al 2019), which followed 29,000 male smokers for 30 years, showed that a better diet with an approximately 30% higher content of natural alpha-tocopherol, initially reduced mortality by 22%, including atherosclerosis by 10-21%, heart attack by 2-17% and cerebral hemorrhage by 22-38%. A supplement of 50 mg/day RL alpha-tocopherol for approximately 6 years within the 30-year period, on the other hand, did not affect symptoms or mortality in the short or long term.
Another long-term American study followed 3,780 healthy women for 11 years, measuring the effect of an alpha-tocopherol supplement to double the level of alpha-tocopherol in the blood. The women were aged between 50 and 79 at the start of the study. The study found an 8% reduced incidence of cerebral hemorrhage with higher levels of alpha-tocopherol in the blood, but an increased incidence of other cardiovascular diseases, such that the overall incidence of cardiovascular problems increased by 8%.
Chemically produced “vitamin E”
Since vitamin E is a strong antioxidant that is known to reduce the unwanted oxidation of LDL cholesterol and other fats in the walls of cells, thereby counteracting atherosclerosis, etc. (Belcher et al 1993), it is relevant to ask why large and long-term studies do not unequivocally show that a supplement of vitamin E is super good.
One explanation could be that we somehow need free radicals, and that vitamin E, with its antioxidant effect, therefore removes something “good.” A more credible explanation, in my perspective, is that large-scale experiments have often used a cheap and poor form of chemically produced vitamin E.
When people talk about there being 8 forms of vitamin E, they are often referring to the 8 different molecules shown above (Figure 1). However, alpha-tocopherol is a complex molecule, and in three places in the molecule a carbon atom is linked to four other atoms/molecules. In the figure below, the positions of the three carbon atoms are marked with red stars (Figure 2).
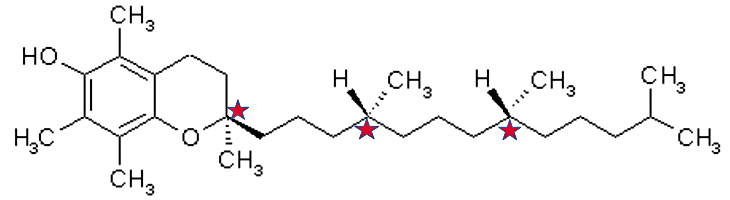
Figure 2: Drawing of the molecular structure of alpha-tocopherol, where the stars mark the three places where a carbon has four different bonds. (Figure modified from Kohlmeier (2015)).
When you look at the drawing, you can easily imagine that the different molecules can rotate freely, but in reality they are very stable. If hydrogen (H) and the methyl molecule (CH3) are in just one of the places opposite to what is shown in the drawing – yes – then biologically you have seen a different molecule.
Unfortunately, this is exactly what happens when you produce vitamin E the old-fashioned chemical way. That is, atoms and molecules turn randomly, which means that they have two possible positions in three different places.
Therefore, 2 different x 2 different x 2 different = a total of 8 different forms of the molecule are chemically produced – see Figure 3 below. Of these, only one form is the natural form of vitamin E, which is found in plants and therefore in our diet, while the other seven versions of the molecule are unknown to plants and animals.
In particular, the four forms shown on the right in the figure below are broken down relatively quickly in the liver like other foreign substances. However, we know very little about what toxic effects they have before they are broken down, and what long-term toxic effects arise due to the more or less broken down substances.

Figure 3: Graphic illustration of the eight forms of vitamin E that are created when attempting to produce vitamin E using simple chemical methods. The natural alpha-tocopherol is marked in red. (Figure modified from Kohlmeier (2015)).
When you want to produce cheap supplements, such as cheap multivitamin pills, you often use chemically produced vitamin E. In these cheap products, the mixture of the eight forms of vitamin E is called rac alpha-tocopherol or DL alpha-tocopherol. The natural alpha-tocopherol has been given first names such as D alpha-tocopherol or RRR alpha-tocopherol.
To increase the shelf life of various foods, vitamin E is often used as an antioxidant during production. Since the focus is on vitamin E’s antioxidant effect and not its effect as a vitamin, many manufacturers prefer to use the cheapest form of vitamin E, which is the chemically produced form that contains all 8 forms in equal amounts.
Figure 4 below graphically shows how the eight natural forms of vitamin E should be understood, compared to the seven additional forms that arise when alpha-tocopherol is produced chemically.
It can be seen that the variation in natural vitamin E is due to variation in the ring shown on the left, while the variation in chemically produced alpha-tocopherols is due to changes in the long chain extending from the rings.

Figure 4: At the top, the eight forms of vitamin E found in plants, and therefore naturally present in our diet, and then the eight forms of alpha-tocopherol – one natural and the other seven forms resulting from the chemical production of alpha-tocopherol, which are therefore also present in our diet when “vitamin E” is used as an antioxidant and in cheap dietary supplements. (The figure is modified from Kohlmeier (2015) and Querchi et al. (2015)).
Conclusion
It is now well documented that the different forms of vitamin E, in addition to their common effect as antioxidants, have quite different mechanisms of action in the body. The different natural forms of vitamin E contribute with different mechanisms to protect the body’s cardiovascular system, the central nervous system and also provide some protective effect against certain forms of cancer.
The chemical production of alpha-tocopherol, on the other hand, casts a shadow over the results achieved with long-term supplementation of alpha-tocopherol, so that it is not possible to determine whether a daily supplement of this vitamin E contributes to a healthy and long life or perhaps has negative effects.
Tocotrienols are always extracted from natural sources, and existing studies show that they have a safe effect even at relatively high daily intakes. It is therefore advantageous to choose a vitamin E with a high content of tocotrienols.
Klaus K. Sall
Biologist, Cand. Scient.
Sall&Sall Counseling
Notes
EFSA: The European Food Safety Authority EFSA estimates that a daily adequate intake of vitamin E measured as alpha tocopherol is 13 mg/day for men and 11 mg/day for women (EFSA 2015). In 2024, EFSA estimated that the highest daily intake for adults is 300 mg D alpha-tocopherol (EFSA 2024). In a previous specific case, EFSA estimated that a daily intake of 1000 mg mixed tocotrienols and tocopherols does not pose risks. (EFSA 2008).
Chirality: The eight forms of alpha-tocopherol that are formed during chemical production – are part of a phenomenon called chiral molecules. I have created a website that describes the importance of this phenomenon for all life (text in Danish): www.kiral.dk.
Mix: Studies have shown that alpha-tocopherol suppresses the body’s use of tocotrienols. Therefore, in supplements containing both alpha-tocopherol and tocotrienols, the tocopherols will be primarily utilized (Querishi et al 2015).
12: A total of 12 natural molecules have been found that have vitamin E effects. Four of them rarely occur in human food and are not known in dietary supplements.
Organic farming: In organic foods, it is not permitted to use the unnatural forms of alpha-tocopherol.
References and further reading
Belcher, J.D. et al. (1993) ‘Vitamin E, LDL, and endothelium. Brief oral vitamin supplementation prevents oxidized LDL-mediated vascular injury in vitro.’, Arteriosclerosis and Thrombosis: A Journal of Vascular Biology, 13(12), pp. 1779–1789. Available at: LINK.
EFSA (2008) ‘Opinion on mixed tocopherols, tocotrienol tocopherol and tocotrienols as sources for vitamin E added as a nutritional substance in food supplements, EFSA Journal, 6(3), p. 640. Available at: https://doi.org/10.2903/j.efsa.2008.640.
EFSA (2015) ‘Scientific Opinion on Dietary Reference Values for vitamin E as α-tocopherol’, EFSA Journal, 13(7), p. 4149. Available at: https://doi.org/10.2903/j.efsa.2015.4149.
EFSA (2024) ‘Scientific opinion on the tolerable upper intake level for vitamin E’, EFSA Journal, 22(8), p. e8953. Available at: https://doi.org/10.2903/j.efsa.2024.8953.
Huang, J. et al. (2019) ‘Relationship Between Serum Alpha-Tocopherol and Overall and Cause-Specific Mortality’, Circulation Research, 125(1), pp. 29–40. Available at: LINK.
Kohlmeier, M. (2015) Fat-Soluble Vitamins and Nonnutrients: Vitamin E, in: Nutrient Metabolism: Structures, Functions, and Genes, pp. 514–525. Elsevier. Available at: LINK.
Qureshi et al. (2015) ‘Pharmacokinetics and Bioavailability of Annatto δ-tocotrienol in Healthy Fed Subjects’, Journal of Clinical & Experimental Cardiology, 6(11). Available at: LINK.
Rafique, S. et al. (2024) ‘Comparative efficacy of tocotrienol and tocopherol (vitamin E) on atherosclerotic cardiovascular diseases in humans’, Journal of the Pakistan Medical Association, 74(6), pp. 1124–1129. Available at: https://doi.org/10.47391/JPMA.9227.
Sen, C. et al. (2000) ‘Molecular basis of Vitamin E action – Tocotrienol potently inhibits glutamate-induced pp60(c-Src) kinase activation and death of HT4 neuronal cells’, The Journal of biological chemistry, 275, pp. 13049–55. Available at: https://doi.org/10.1074/jbc.275.17.13049.
Sen, C.K. et al. (2007) ‘Tocotrienols: The Emerging Face of Natural Vitamin E’, Vitamins and hormones, 76, p. 203. Available at: https://doi.org/10.1016/S0083-6729(07)76008-9.